动脉粥样硬化可累及全身多部位血管[1],其中颈动脉和冠状动脉并存动脉粥样硬化性狭窄的发生率越来越高,有文献[2]报道心绞痛人群中颈动脉狭窄的发病率可达54.5%,其中10%的患者需要进行手术干预;而重度颈动脉狭窄患者中约12%需要行冠状动脉旁路移植术(coronary artery bypass grafting,CABG)[3]。对于这种类患者,同期或分期颈动脉内膜剥脱术(carotid endarterectomy,CEA)及CABG报道了不错的效果[4],颈动脉支架术(carotid artery stenting,CAS)微创,并且一些随机对照研究报道了不劣于CEA的疗效[5-7],随着技术及器械的发展,其也被逐渐应用到颈动脉狭窄合并冠心病患者的颈动脉血运重建中[8]。本研究回顾了中日友好医院心脏血管外科2007年1月—2014年12月行同期或分期CAS和CABG患者临床资料,现报告如下。
1 资料与方法
1.1 一般资料
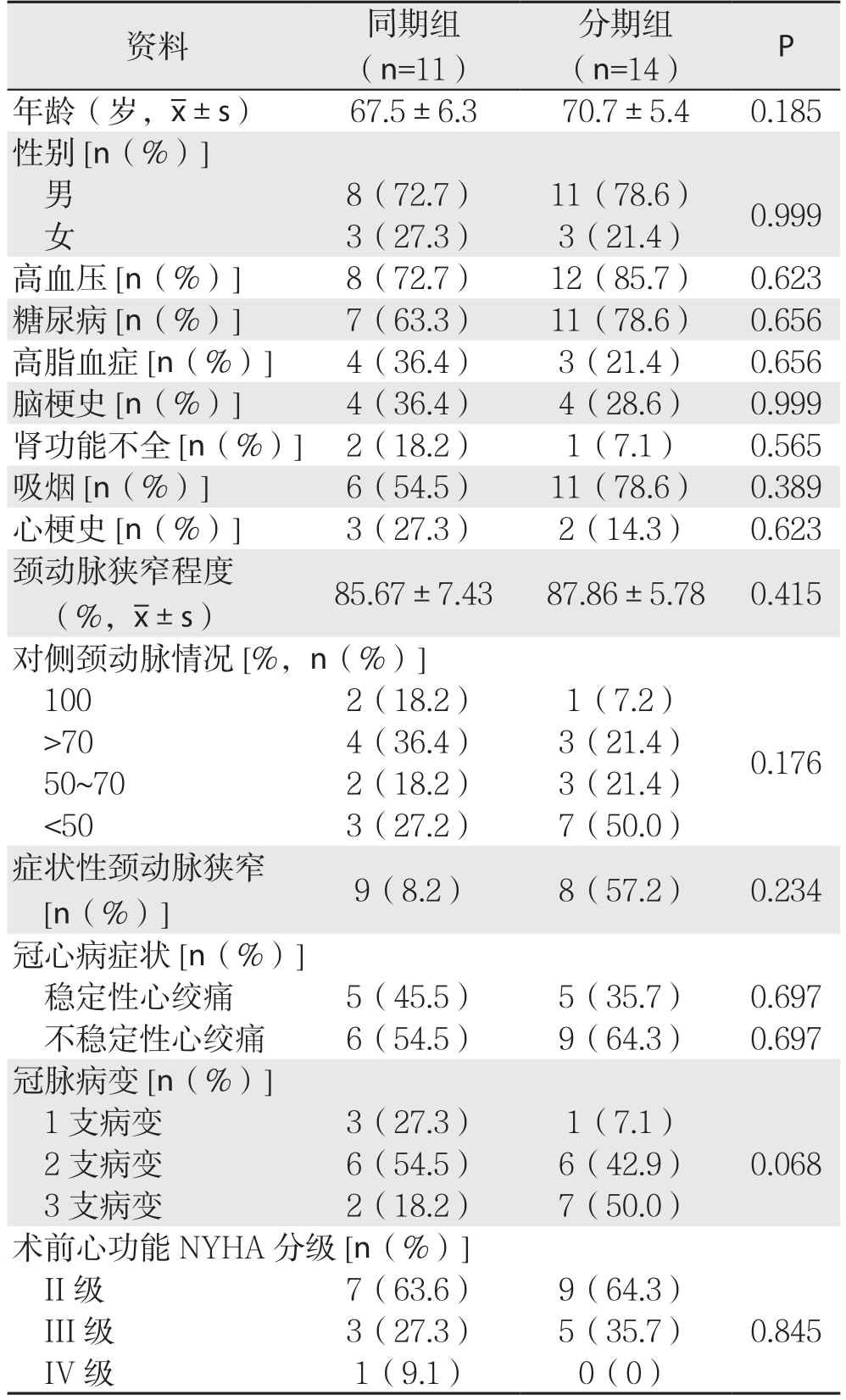
2007年1月—2014年12月,中日友好医院心脏血管外科共收治颈动脉狭窄合并冠心病患者75例,同期或分期行CAS与CABG者25例,其中同期11例,分期14例。25例患者中男19例,女6例;年龄55~80岁,平均(69.3±7.5)岁;合并高血压20例,糖尿病18例,高脂血症7例;吸烟17例;患者均经冠状动脉造影明确冠状动脉病变,冠状动脉3支病变者9例,2支病变者12例,1支病变者4例,累及左主干者8例;既往心肌梗死患者5例,不稳定性心绞痛15例,稳定性心绞痛10例;经颈动脉超声、计算机断层扫描血管造影(CTA)和(或)数字减影血管造影(DSA)明确颈动脉狭窄程度,颈动脉中度狭窄(50%~69%)7例,重度狭窄(70%~99%)18例;症状性颈动脉狭窄17例,主要症状包括肢体感觉和(或)运动障碍、黑朦、失语及6个月内的一过性脑缺血发作,无症状性颈动脉狭窄8例;根据颈动脉支架术和冠状动脉旁路移植术施行时序的不同,分为同期组和分期组,其中同期组11例(男8例,女3例),平均年龄(67.5±6.3)岁;分期组14例(男11例,女3例),平均年龄(70.7±5.4)岁。两组患者的基本资料见表1。
1.2 纳入排除标准
纳入标准:⑴ 颈动脉超声、CTA或DSA证实症状性颈动脉狭窄≥50%,无症状性颈动脉狭窄≥70%;⑵ 冠状动脉DSA证实冠状动脉有行冠状动脉旁路移植术的指征;⑶ 同期或者分期行颈动脉支架和冠状动脉旁路移植手术者。排除标准:⑴ 行同期或者分期颈动脉内膜剥脱术和冠状动脉旁路移植术者;⑵ 未行手术治疗者。
表1 两组患者的基本资料
Table 1 General data of the two groups of patients
1.3 治疗方法
双侧颈动脉狭窄者优先处理症状侧,双侧均无症状则优先处理狭窄程度重的一侧,当一过性脑缺血发作(transient ischemia attack,TIA)或缺血性脑卒中患者无早期颈动脉血运重建禁忌证时,争取在2周内进行手术[9],CAS中常规应用远端脑保护装置。冠状动脉搭桥均在心脏跳动下进行,若患者存在急性心梗则在心梗6周后进行手术,对部分血流动力学不稳定者术前自股动脉置入主动脉内球囊反搏导管(intra-aortic balloon pump,IABP)。
同期手术者术前给予阿司匹林100 mg/d,至少3 d,术后尽快给予阿司匹林100 mg/d并长期服用,同时给予氯吡格雷75 mg/d,持续6个月。分期手术者颈动脉支架术前给予阿司匹林100 mg/d,至少3 d,术后给予阿司匹林100 mg/d及氯吡格雷75 mg/d,CABG术前3 d停用氯吡格雷,术后尽快给予阿司匹林100 mg/d并长期服用,同时给予氯吡格雷75 mg/d,持续6个月。
手术均在复合手术室完成,采用气管插管静吸复合全身麻醉,单纯颈动脉支架术采用局部麻醉。CAS过程:Seldinger法穿刺股动脉,经血管鞘放入造影导管及导丝,交换长鞘至颈总动脉,放置保护伞至颈内动脉颅内段,沿导丝置入球囊并行预扩张,而后根据颈动脉尺寸及病变长度置入支架,根据造影结果决定是否进行后扩张,残余狭窄≤30%视为治疗成功[10],最后应用血管缝合器缝合穿刺点。CABG过程:术中全身肝素化,保持激活全血凝固时间(activated clotting time,ACT)>250 s,采用胸骨正中切口,劈开胸骨并打开心包后,悬吊心包,显露心脏及主动脉根部,移植血管选用乳内动脉或者大隐静脉,使用乳内动脉者首先游离左侧乳内动脉,远端吻合至前降支;使用大隐静脉者,获取大隐静脉后,首先使用侧壁钳钳夹主动脉侧壁,并使用打孔器在主动脉侧壁打孔,先进行近心端吻合,之后行单支或序贯远端吻合,检查移植血管通畅后,硫酸鱼精蛋白中和肝素后确切止血并逐层关闭切口。
1.4 统计学处理
数据采用SPSS 22统计学软件处理,计量资料如符合正态分布,用均数±标准差( ±s)表示,两组间比较应用两独立样本t检验;如不符合正态分布,则用中位数和四分位数间距[M(Q1~Q3)]表示,两组间比较应用非参数检验(Wilcoxon秩和检验)。计数资料的比较应用χ2检验或者Fisher精确概率法。两组间对侧颈动脉狭窄程度及冠状动脉病变程度的比较采用秩和检验。检验水准α=0.05。
±s)表示,两组间比较应用两独立样本t检验;如不符合正态分布,则用中位数和四分位数间距[M(Q1~Q3)]表示,两组间比较应用非参数检验(Wilcoxon秩和检验)。计数资料的比较应用χ2检验或者Fisher精确概率法。两组间对侧颈动脉狭窄程度及冠状动脉病变程度的比较采用秩和检验。检验水准α=0.05。
2 结 果
2.1 手术结果
本组患者共进行70条冠状动脉重建,平均每个患者2.8条;共置入颈动脉支架25枚,平均每个患者1枚。同期手术11例(8例先CAS,后CABG;3例先CABG,后CAS),其中1例患者在CAS后准备行CABG时出现室颤,经电除颤后恢复并完成手术;分期手术14例(5例先CAS,后CABG;9例先CABG,后CAS)。16例患者在术前置入IABP(同期组7例,分期组9例),2例同时行冠状动脉支架置入(分期组2例),2例合并肾动脉狭窄同时行肾动脉支架置入术(同期组1例,分期组1例),3例合并髂动脉狭窄同时行髂动脉支架植入术(同期组1例,分期组2例)。
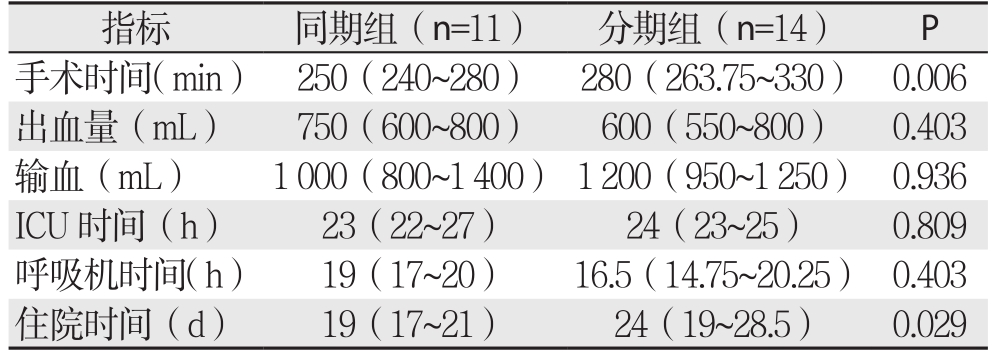
与分期组比较,同期组中位手术时间(250 min vs.280 min)、中位住院时间(19 d vs. 24 d)明显缩短(均P<0.05),中位术中出血量(750 mL vs. 600 mL)、输血量(1 000 mL vs. 1 200 mL)、ICU时间(23 h vs.24 h)、呼吸机时间(19 h vs. 16.5 h)差异均无统计学意义(均P>0.05)(表2)。
2.2 并发症及处理
同期组术后30 d内出现小卒中1例(9.1%),TIA 1例(9.1%),术后短暂低血压3例(27.3%),围手术期肺部感染1例(9.1%),无心肌梗死及死亡病例;分期组术后呼吸机应用中位时间为16.5 h,中位住院时间24 d,术后30 d内出现TIA 2例(14.3%),术后短暂低血压4例(28.6%),再次开胸止血1例(7.1%),围手术期肺部感染1例(7.1%),无心肌梗死及死亡病例。
表2 两组患者围手术期主要临床指标比较[M(Q1~Q3)]
Table 2 Comparison of the main perioperative variables between the two groups of patients [M (Q1-Q3)]
2.3 随访结果
25例患者中21例获随访,随访率为84%,随访时间为14~112个月,平均随访53个月。同期组1例患者术后1年因癌症死亡,1例术后2年因心梗死亡;分期组1例患者术后4年因心功能不全死亡。
3 讨 论
随着生活习惯的改变,中风和心血管疾病已成为国内导致死亡的两大原因[11],动脉粥样硬化可以同时引起颈动脉和冠状动脉狭窄,Chen等[12]报道颈动脉狭窄患者发生心血管事件的风险明显增加,同时大量的研究[2,13]也报道冠心病患者中颈动脉狭窄的发生率可达20%~54.5%。尽管颈动脉狭窄合并冠心病的发病率较高,但对这类患者的处理仍存在很大的争议,先行冠状动脉血运重建往往会增加脑卒中的发生率,而先行颈动脉血运重建往往会增加心梗的发生率,为同时解决颈动脉狭窄和冠心病的问题,减少围手术期并发症,有学者[14-15]提出同期进行冠状动脉和颈动脉血运重建,因其可以减少分次手术导致的围手术期心肌梗死和脑卒中的风险,同时可以避免二次麻醉的打击,减少住院天数和费用。
自1951年Debakey成功实施第1例CEA后,其逐渐成为治疗颈动脉狭窄最常用的方法,这种传统的手术方法同样适用于需行CABG同时合并颈动脉狭窄的患者,Sharma等[15]回顾了17 469例同期CEA+CABG手术,证实了这种术式的可行性和安全性。随着材料、影像技术和介入技术的发展以及栓子保护装置的应用,颈动脉支架术的安全性和有效性逐渐被认可,尤其是对于存在冠心病等高危因素的患者,其微创、恢复快的特点也有很大的优势,因此其在冠心病合并颈动脉狭窄患者颈动脉血运重建方面的应用逐渐增多[8,16-18],Shishehbor等[19]报道在颈动脉与冠状动脉同期血运重建时,与CEA相比,CAS的远期效果要更好一些。因此,笔者对于颈动脉斑块较稳定、钙化较轻、同时解剖条件适合的患者行CAS。本组患者中同期与分期CAS及CABG均取得了较好的治疗效果,但同期手术缩短了手术和住院时间,具有一定的优势。
目前同期颈动脉和冠状动脉血运重建手术的适应证还没有达成共识。Barrera等[20]选择无症状性颈动脉狭窄患者进行同期手术,而Dzierwa等[21]对症状性颈动脉狭窄患者进行同期手术,都取得了不错的效果。对于患者的选择,笔者的经验是:对于年龄>50岁,因冠心病或颈动脉狭窄就诊的患者,常规行颈动脉和冠状动脉CTA或DSA检查,以明确是否有合并病变。若症状性颈动脉狭窄≥50%,无症状性颈动脉狭窄≥70%,同时冠状动脉有血运重建指征,且心功能良好者可行同期手术,对于心功能较差者可考虑行同期手术,但术前应放置IABP导管。
对于同期CAS和CABG手术顺序问题,目前没有定论。为预防CABG术中搬动心脏引起血流动力学不稳定导致脑缺血,有的学者选择先行CAS[22],本组患者中1例在置入颈动脉支架准备行CABG时突然出现室颤,可能是由于支架置入后刺激颈动脉窦,引起颈动脉窦反射,从而导致血流动力学不稳定。因此,对于多数患者,笔者选择先行CAS,而对于心脏功能相对不稳定者,选择先行CABG。
同期手术者,围手术期抗血小板药物的应用比较统一,一般是术前给予阿司匹林,术后尽快给予阿司匹林及氯吡格雷。而对于分期手术者,围手术期抗血小板药物的应用尚无统一的标准,且争议较大[23],美国心脏学会(American Heart Association,AHA)指南建议CABG术前继续应用阿司匹林,并在术后6 h内恢复应用[24],但为了避免围手术期出血风险增加,CABG术前应停用氯吡格雷[25]。本组患者中如果先行CAS,则CABG术前继续应用阿司匹林,但是停用氯吡格雷至少3 d。所有患者中,分期组有1例术后需再次开胸止血,其余均无大出血现象。
总之,同期和分期CAS及CABG在颈动脉狭窄合并冠心病的治疗中都安全有效,同期手术可以缩短手术和住院时间,应根据患者的病变特点选择合适的治疗方法。
参考文献
[1]Ross R. Atherosclerosis--an inflammatory disease[J]. N Engl J Med,1999, 340(2):115–126.
[2]Zhang J, Xu R, Liu P, et al. Prevalence of carotid artery stenosis in Chinese patients with angina pectoris[J]. J Thorac Dis, 2015,7(12):2300–2306. doi: 10.3978/j.issn.2072–1439.2015.12.42.
[3]Steinvil A, Sadeh B, Arbel Y, et al. Prevalence and predictors of concomitant carotid and coronary artery atherosclerotic disease[J]. J Am Coll Cardiol, 2011, 57(7):779–783. doi: 10.1016/j.jacc.2010.09.047.
[4]Naylor AR, Cuffe RL, Rothwell PM, et al. A systematic review of outcomes following staged and synchronous carotid endarterectomy and coronary artery bypass[J]. Eur J Vasc Endovasc Surg, 2003,25(5):380–389.
[5]Brott TG, Hobson RW, Howard G, et al. Stenting versus endarterectomy for treatment of carotid-artery stenosis[J]. N Engl J Med, 2010, 363(1):11–23. doi: 10.1056/NEJMoa0912321.
[6]原野, 郭大乔, 符伟国, 等. 颈动脉内膜剥脱与支架置入术患者围手术期脑灌注对比分析[J]. 中国普通外科杂志, 2015,24(12):1727–1731. doi:10.3978/j.issn.1005–6947.2015.12.017.Yuan Y, Guo DQ, Fu WG, et al. Carotid endarterectomy versus carotid artery stenting on cerebral perfusion in patients with carotid stenosis[J]. Chinese Journal of General Surgery, 2015, 24(12):1727–1731. doi:10.3978/j.issn.1005–6947.2015.12.017.
[7]刘鹏, 樊雪强, 叶志东. 颈动脉内膜切除术和支架植入术的合理选择[J]. 中国普通外科杂志, 2014, 23(6):715–718. doi:10.7659/j.issn.1005–6947.2014.06.001.Liu P, Fan XQ, Ye ZD. Rational choice of carotid endarterectomy and carotid artery stenting[J]. Chinese Journal of General Surgery,2014, 23(6):715–718. doi:10.7659/j.issn.1005–6947.2014.06.001.
[8]浮志坤, 董自超, 杜虹, 等. 冠状动脉旁路移植术和颈动脉支架术治疗冠心病合并颈动脉狭窄[J]. 中国医师杂志, 2015, 17(1):128–130. doi:10.3760/cma.j.issn.1008–1372.2015.01.044.Fu ZK, Dong ZC, Du H, et al. Coronary artery bypass grafting and carotid artery stenting for coronary disease and concomitant carotid stenosis[J]. Journal of Chinese Physician, 2015, 17(1):128–130.doi:10.3760/cma.j.issn.1008–1372.2015.01.044.
[9]吉训明, 吴川杰. 急性脑梗死后颈动脉血运重建手术时机的探讨[J]. 中华神经外科杂志, 2017, 33(4):325–327. doi:10.3760/cma.j.issn.1001–2346.2017.04.001.Ji XM, Wu CJ. Timing for carotid artery recanalization after acute cerebral infarction[J]. Chinese Journal of Neurosurgery, 2017,33(4):325–327. doi:10.3760/cma.j.issn.1001–2346.2017.04.001.
[10]高峰, 杜彬, 秦海强, 等. 2007年颈动脉支架成形术专家共识[J]. 中国卒中杂志, 2007, 2(5):430–454. doi:10.3969/j.issn.1673–5765.2007.05.017.Gao F, Du B, Qin HQ, et al. 2007 Clinical Expert Consensus Document on Carotid Stenting[J]. Chinese Journal of Stroke, 2007,2(5):430–454. doi:10.3969/j.issn.1673–5765.2007.05.017.
[11]Liu L, Wang D, Wong KS, et al. Stroke and stroke care in China:huge burden, significant workload, and a national priority[J]. Stroke,2011, 42(12):3651–3654. doi: 10.1161/STROKEAHA.111.635755.
[12]Chen PC, Jeng JS, Hsu HC, et al. Carotid Atherosclerosis Progression and Risk of Cardiovascular Events in a Community in Taiwan[J]. Sci Rep, 2016, 6:25733. doi: 10.1038/srep25733.
[13]Kazum S, Eisen A, Lev EI, et al. Prevalence of Carotid Artery Disease among Ambulatory Patients with Coronary Artery Disease[J]. Isr Med Assoc J, 2016, 18(2):100–103.
[14]张乐峰, 武恒朝, 孙寒松, 等. 同期或分期行颈动脉支架置入术与非体外循环冠状动脉旁路移植术治疗冠心病合并颈动脉狭窄[J]. 中华胸心血管外科杂志, 2012, 28(1):20–23. doi:10.3760/cma.j.issn.1001–4497.2012.01.007.Zhang LF, Wu HC, Sun HS, et al. Simultaneous hybrid or staged carotid artery stenting and off-pump coronary artery bypass for treatment of coronary artery disease in patients with concomitant severs carotid artery stenosis[J]. Chinese Journal of Thoracic and Cardiovascular Surgery, 2012, 28(1):20–23. doi:10.3760/cma.j.issn.1001–4497.2012.01.007.
[15]Sharma V, Deo SV, Park SJ, et al. Meta-analysis of staged versus combined carotid endarterectomy and coronary artery bypass grafting[J]. Ann Thorac Surg, 2014, 97(1):102–109. doi: 10.1016/j.athoracsur.2013.07.091.
[16]Velissaris I, Kiskinis D, Anastasiadis K. Synchronous carotid artery stenting and open heart surgery[J]. J Vasc Surg, 2011, 53(5):1237–1241. doi: 10.1016/j.jvs.2010.11.049.
[17]Randall MS, Mckevitt FM, Cleveland TJ, et al. Is there any benefit from staged carotid and coronary revascularization using carotid stents? A single-center experience highlights the need for a randomized controlled trial[J]. Stroke, 2006, 37(2):435–439.
[18]中国医疗保健国际交流促进会血管疾病高血压分会专家共识组. 冠心病合并颈动脉狭窄的处理策略专家共识[J]. 中国循环杂志, 2016, 31(12):1150–1156. doi:10.3969/j.issn. 1000–3614.2016.12.002.Expert Consensus Group of Hypertension Branch of Vascular Disease Society of China International Exchange and Promotive Association for Medical and Health Care. Expert Consensus on treatment of coronary disease and concomitant carotid stenosis[J].Chinese Circulation Journal, 2016, 31(12):1150–1156. doi:10.3969/j.issn.1000–3614.2016.12.002.
[19]Shishehbor MH, Venkatachalam S, Sun Z, et al. A direct comparison of early and late outcomes with three approaches to carotid revascularization and open heart surgery[J]. J Am Coll Cardiol,2013, 62(21): 1948–1956. doi: 10.1016/j.jacc.2013.03.094.
[20]Barrera JG, Rojas KE, Balestrini C, et al. Early results after synchronous carotid stent placement and coronary artery bypass graft in patients with asymptomatic carotid stenosis[J]. J Vasc Surg,2013, 57(2 Suppl):58S-63S. doi: 10.1016/j.jvs.2012.06.116.
[21]Dzierwa K, Pieniazek P, Musialek P, et al. Treatment strategies in severe symptomatic carotid and coronary artery disease[J]. Med Sci Monit, 2011, 17(8):RA191–197.
[22]Versaci F, Reimers B, Del Giudice C, et al. Simultaneous hybrid revascularization by carotid stenting and coronary artery bypass grafting: the SHARP study[J]. JACC Cardiovasc Interv, 2009,2(5):393–401. doi: 10.1016/j.jcin.2009.02.010.
[23]Dong H, Jiang X, Peng M, et al. The interval between carotid artery stenting and open heart surgery is related to perioperative complications[J]. Catheter Cardiovasc Interv, 2016, 87(Suppl 1):564–569. doi: 10.1002/ccd.26408.
[24]Hillis LD, Smith PK, Anderson JL, et al. 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines[J]. J Am Coll Cardiol, 2011, 58(24):e123–210. doi: 10.1016/j.jacc.2011.08.009.
[25]Herman CR, Buth KJ, Kent BA, et al. Clopidogrel increases blood transfusion and hemorrhagic complications in patients undergoing cardiac surgery[J]. The Ann Thorac Surg, 2010, 89(2):397–402. doi:10.1016/j.athoracsur.2009.10.051.
